 |
 |
Occlusion of the retinal artery may be caused by arteriosclerotic
changes, embolus
(from heart or carotid artery) or inflammation (rare)
History:
- Sudden painless visual loss which may be complete (due to central retinal artery
- Patient usually have a history of hypertension or heart disease
occlusion) or partial (due to branch retinal artery occlusion)
- The visual acuity is reduced in central retinal artery occlusion but may be normal
- Relative afferent pupillary defect is present in central retinal artery occlusion
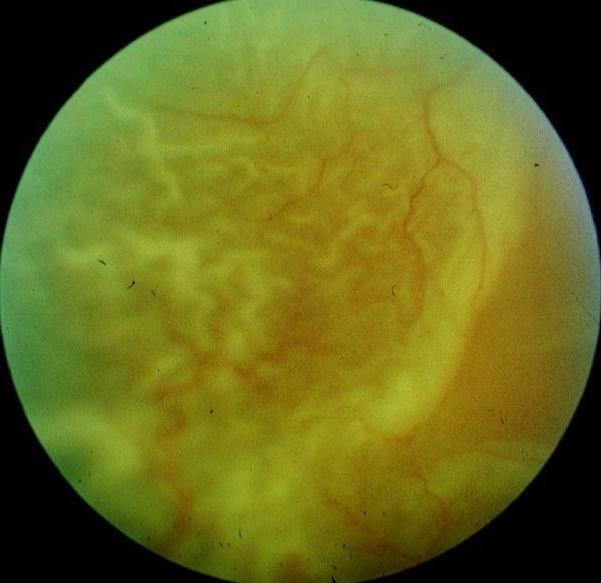
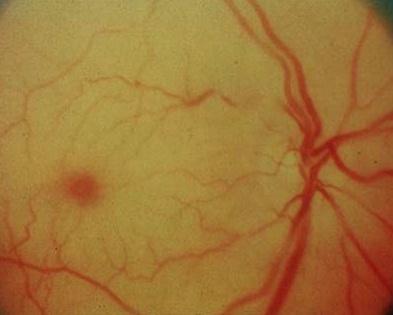
- The retinal arteries are narrow or collapsed.
- In central retinal artery occlusion, the fovea shows a cherry-red spot against the
- In branch retinal artery occlusion, the white infarcted retina corresponds to the
- Emboli may be seen in the arteries if the cause is emboli
in branch retinal artery occlusion
white infarcted retina.
occluded retina.
- Immediate referral if the visual loss is less than 6 hours as treatment may restore
- Treatment involves the use of intravenous acetazolamide and globe massage to
- Further management aim to uncover any underlying diseases such as hypertension,
- Long term low dose aspirin is advised to reduce the risk of occurrence.
some or most of the function.
lower the intraocular pressure and hopefully re-establish the arterial flow.
cardiac or carotid thrombus. An ESR is usually performed in the absence of obvious
embolus to exclude arteritic causes.