1. What is fluorescein angiography?
2. What kind of substance is sodium fluorescein?
3. How is fluorescein angiography performed?
4. What are the side effects of fluorescein
angiography?
5. How do ocular structures determine the distribution
of fluorescein
angiography?
6. What are the phases of a normal fluorescein
angiography.
7. List some of the main indications for fluorescein
angiography.
1. What is fluorescein angiography?
It is a fundal photography,
performed in rapid sequence following intravenous injection of fluorescein
dye.
It provides three main information:
a. the flow characteristics
in the blood vessels as the dye reaches
and circulates
through the retina and choroid
b. it records fine details of the
pigment epithelium and retinal
circulation
that may not otherwise be visible
c. give a clear picture of the
retinal vessels and assessment of their
functional integrity.
2. What kind of substance is sodium
fluorescein?
Sodium fluorescein (C20H10O5Na2)
is an organic dye. It has a molecular weight of 376 daltons, and is 80%
bound to plasma albumin. The remaining 20% is seen during angiography.
The dye absorbs light in the blue range of the visible spectrum, with absorption
peaking at 490nm (blue). It emits light at 530nm (yellow).
It is metabolized by the liver
and excreted by the kidneys. Most dye is cleared with 24 hours and patients
should be warned that their urine will appear orange during this time.
3. How is fluorescein angiography
performed?
5ml of 10% sodium fluorescein
dye is injected as a bolus into the vein (preferably antecubital) of the
patient's arm.
The eye is illuminated using blue
light produced by a blue filter (excitation filter). The fundus is viewed
through a yellow filter (barrier filter). As blue light cannot pass through
a yellow filter in normal circumstances nothing can be seen. However, fluorescein
dye within retinal and choroidal blood vessels absorbs blue light and emits
yellow light, this yellow light passes through the filter and is photographed.
Only tissues that contains fluorescein are visualized.
4. What are the side effects of fluorescein
angiography?
The side effects include:
-
Those which are unavoidable such as
a temporary tan skin colour form the dye, red after image from the photoflash
and discoloration of the urine
-
Nausea and vomiting (10%). Usually
transient and no treatment is usually needed.
-
Vasovagal synocope (1%) and no treatment
is needed. But in extreme bradycardia, IV atropine may be needed.
-
Anaphylaxis such as bronchospasm, urticarial
skin rash and hypotension (<1%). Treatment is with chlorpheniramine
(piriton) 10mg IV, hydrocortisone 100mg IV and give oxygen and adrenaline
1ml of 1:1000 IM for hypotension and bronchospasm.
-
Cardiac and respiratory arrest (<0.01%).
Treatment would involve cardiopulmonary resuscitation.
5. How do ocular structures determine the
distribution of fluorescein angiography?
Fluorescein cannot diffuse
through tight cellular junctions. These are present at two sites within
the fundus:
-
retinal blood vessel endothelium
-
retinal pigment epithelium.
There are two circulation within the
fundus:
-
Choroidal circulation -
the fluorescein freely leaks out
of the fenestrated choroidal capillaries, and from there through Bruch's
membrane. however, tight junctions between retinal pigment epithelium (RPE)
cells prevents dye reaching the retina
-
Retinal circulation -
the retinal blood vessel endothelial
cells are joined by tight junctions which prevent leakage of fluorescein
into the retina. This constitutes the blood retina barrier. Any leakage
from the retinal vessels is abnormal
Capillaries in the ciliary
process re permeable to fluorescein, so dye rapidly appears in the aqueous
following intravenous injection. Fluorescein in the aqueous and vitreous
emits yellow light which reflects off white structures within the eye causing
these structures to falsely appear fluorescent. The optic disc, myelinated
fibres and hard exudates appear progressively more pseudofluorescent through
the course of an angiogram for this reason.
6. What are the phases of a normal fluorescein
angiography?
Normally 10-15 seconds
elapse between dye injection and arrival of dye in the short ciliary arteries.
Choroidal circulation precedes retinal circulation by 1 second. Transit
of dye through the retinal circulation takes approximately 15 to 20 seconds.
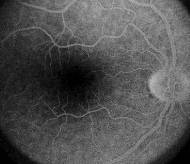
Normal angiogram can be divided
into five phases (see the pictures below)
1. Choroidal phase -
choroidal filling via the
short ciliary arteries results in initial patching filing of lobules, very
quickly followed by a diffuse (blush) as dye leaks out of the choroidocapillaris.
Cilioretinal vessels and prelaminar optic disc capillaries fill during
this phase.
2. Arterial phase -
the central retinal artery
fills about 1 second later than choroidal filling
3. Capillary phase-
the capillaries quickly
fill following the arterial phase. The perifoveal capillary network is
particular prominent as the underlying choroidal circulation is masked
by luteal pigment in the retina and melanin pigment in the RPE. At the
centre of this capillary ring is the foveal avascular zone 500um in diameter.
4. Venous phase -
early filling of the veins
is from tributaries joining their margins, resulting in a tramline effect.
Later the whole diameter of the veins is filled.
5. Late phase -
after 10 to 15 minutes
little dye remains within the blood circulation. Dye which has left the
blood to ocular structures is particularly visible during this phase.
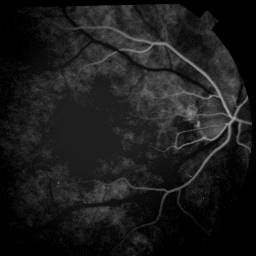
Arterial phase |
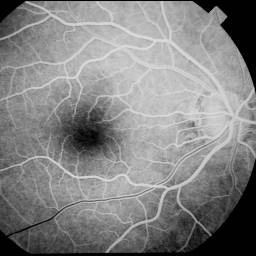
Early venous phase |
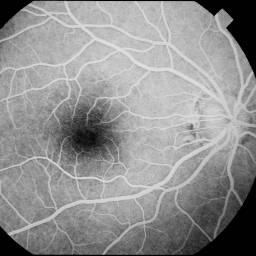
Venous phase |
Late phase |
7. List some of the main indications
for fluorescein angiography.
Fluorescein angiography is used mainly for the study
of abnormal ocular vasculature. The following are the main indications
for fluorescein angiography:
Diabetic mellitus:
-
detecting any significant macular oedema which is not clinically
obvious;
-
locating the area of oedema for laser treatment;
-
differentiating ischaemic from exudative diabetic maculoplathy;
-
differentiating between IRMA and new blood vessels if clinical
differentiation is difficult.
Retinal vein occlusion:
-
determining the integrity of the foveal capillary bed and
the extent of macular oedema following branch retinal vein occlusion
-
differentiating collaterals from neovascularization (see
pictures below)
-
less commonly it is used purely to determine the extent of
retinal ischaemia (as this can be done clinically)
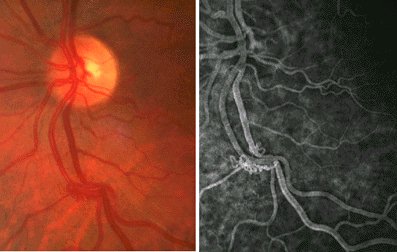
FFA is used to determine if the abnormal blood vessels
are collaterals or neovascularization following branch retinal vein occlusion.
The absence
of dye leakage is in favour of collaterals and sectoiral
photocoagulation
is therefore not indicated. |
Age-related macular degeneration
-
locate the subretinal neovascularization and determine its
suitability for laser treatment.
Other indications:
-
Locating subretinal neovascular membrane in various
conditions (high myopia, angioid streaks, choroidal rupture and chorioretinitis)
-
Locating abnormal blood vessels (for example idiopathic
retinal telangietasia, retinal retinopathy etc)
-
Looking for break down of RPE tight junctions (central
serous retinal retinopathy) or the blood retinal barrier (cystoid
macular oedema)
-
Help with diagnosis of retinal conditions (for example
Stargardt's disease gives a characteristic dark choroid).
|