1. Planning the operation is the first stage to satisfactory
operative outcome.
2. Here are some guidelines for excision of a skin lesion:
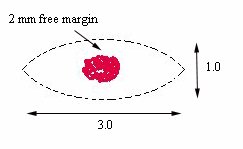
Figure 1 |
-
A spindle-shaped incision circumscribing the lesion is the
best way of removing a lesion
(figure 1).
h
-
To allow neat skin closure, the long axis of the incision
should measure not less than three times that of the transverse diameter.
-
To ensure complete excision of the lesion, a narrow strip
of normal skin on either side of the lesion is excised.
-
Where possible the incisions should be placed so that the
scar will lie in a line of election (the lines that give the least stretching).
This means that the long axis of the incision should be aligned with existing
skin creases or wrinkles (nasolabial fold, glabellar wrinkle, lateral canthal
"crow feet" and the forehead wrinkles). In the absence of creases or wrinkles,
the patient can be asked to simulate the appropriate facial expression
such as smiling, frowing or closing the eyes tightly. These manouvres will
make prominent the potential lines.
a
Exceptions to the above:
-
For malignant skin tumour, a clear margin of more than 2
mm is required. For example in basal cell carcinoma 3 mm clear margin is
recommended and in squamous cell carcinoma a margin of 5 mm is recommended.
-
In patients without excess skin as in the young patients,
a conservative policy is desirable in benign skin lesion. This will avoid
the problem of scar contracture. The patient is warned about the risk of
recurrence.
-
In patients without excess skin and the lesion is large but
benign (such as skin naevus, sebrorrheic warts). Serial excision at regular
interval is recommended. This avoids the risk of wound contracture or the
need for skin graft.
While it is desirable to place the incision along the
line of election, it may not appropriate in some cases. The obvious example
is excising a lesion under the lower lid. In patients with lax lid margin,
the subsequent contracture can lead to ectropion. In such cases, an incision
with the long axis perpendicular to the lid margin may be desirable.
3. Mark the proposed incision using a skin marker pen before infiltrating
the site with
local anaesthetic. Infiltration before marking will
distort the tissue.
4. The skin is kept under tension at right angles to the line of incision
using the thumb and
forefinger of the free hand.
5. The incision is made by holding the knife at right angles to the
skin surface (figure 2).
In hair bearing area such as the eyebrow,
the
incision plane should be parallel to the
emergent angle of the hair follicles (figure
3) to facilitate accurate closure.
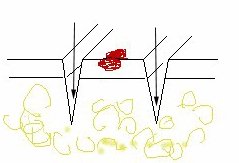
Figure 2. Arrow indicate the plane of
incision. |
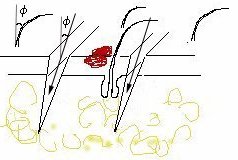
Figure 3. f isthe
angle of the plane of incision which is parallel to the hair follicles |
6. Incise the skin with a confident single stroke so that the
blade penetrate the fatty
subcutaneous layer but not the deep fascia.
|