In the examination, gross specimen rather than histological
slide of optic nerve glioma is likely to be given for discussion.
The following are the key points on optic nerve glioma that the examiner
would expect you to know:
-
a disease of childhood and most patients present
before the age of 10
-
associated with type I neurofibromatosis in
60% of patients
-
present with decreased vision, proptosis or strabismus
-
tumour is fusiform in appearance and causes
optic foramen enlargement
-
slow growing tumour
-
histologically, presence of pilocystic (hair-like)
tumour cells (astrocytoma) and Rosenthal fibres.
Cystic spaces may be present.
-
may be confused with meningioma as it can extend into the meninges causing
meningeal
hyperplasia
A bisected gross specimen of an eye with optic nerve
glioma.
The fusiform appearance is typical of optic nerve glioma.
|
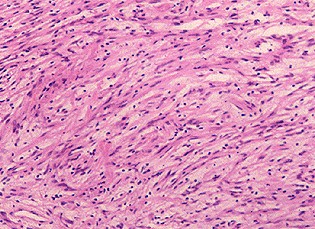
The tumour cells in optic nerve glioma have elongated
or hair-like
appearance (pilocystic).Hence the name pilocystic astrocytoma. |
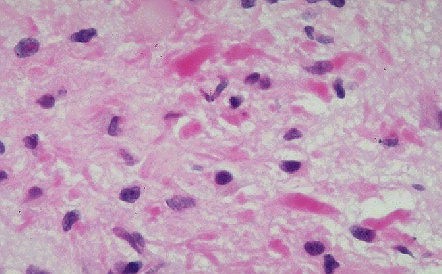
Rosenthal fibres in optic nerve glioma. These are degenerative
eosinophilic substances found within the cytoplasm of
astrocytes.
There are characteristic but not diagnostic of optic
nerve glioma.
|
Common viva questions:
-
How does optic nerve glioma differ from optic nerve meningioma?
-
What may cause a sudden increase in proptosis in a patient with known optic
nerve glioma? (Malignant transformation or coalescence of cystic spaces.)
|