Actinic (solar) keratosis and solar keratosis are two common
conditions seen in sun-damaged skin. They are commonly seen around the
eye. However, the two conditions are histologically different and have
different clinical importance.
Clinically, actinic (solar) keratosis appears as ill-defined erythematous
macules or papules with scaly surface. It can progress to squamous cell
carcinoma if untreated.

Solar keratosis in the left lower lid with
erythematous and scaly surface. |

Solar keratosis of the nose below the right medial
canthus. |
Histologically, the following features are noted (note: the
main feature of actinic keratosis is dysplasia without invasion):
-
hyperkeratosis (increased amount of keratin)
-
parakeratosis (presence of cell nuclei in
the keratin layer, this is a sign of decreased turnover time of the epidermis)
-
dysplasia (abnormal maturation of the epidermis;
the cells have atypical morphology cytologically)
-
solar elastosis (in which the dermis is stained
blue rather than pink resembling the elastic tissue; this is a sign of
sun damage)
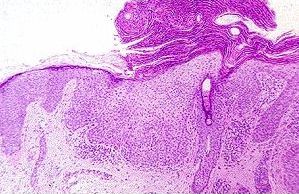
Actinic keratosis with all the typical features:
hyperkeratosis, parakeratosis, dysplasia and solar keratosis. |
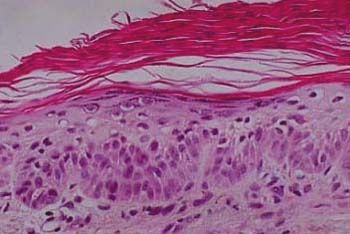
Higher magnification showing dysplasia in actinic keratosis. |
Seborrheic keratosis appears as sharply demarcated, black or
brownish in color, and slightly raised lesions, most of them have a verrucous
surface. The condition is benign and malignant transformation is rare.
Removal is mainly for cosmesis.

A large seborrheic keratosis (wart). |

Multiple seborrheic keratosis (warts) |
Histologically, seborrheic keratosis has the following features:
-
the base of the seborrheic keratosis is flat and level with the base of
the adjacent normal epidermis (ie. an exophytic appearance
if the adjacent normal epidermis is included)
-
acanthosis (thickening of the epidermal layer;
in seborrheic keratosis this results from basaloid cell proliferation.
Dysplasia is absent)
-
hyperkeratosis (excess keratin)
-
epidermal cysts filled with keratin (horn cyst)
are common, some of these cysts resulted from infoldings of the epidermis
(pseudohorn cysts).
-
hyperpigmentation of the basaloid cells from
melanin phagocytosis
-
solar elastosis
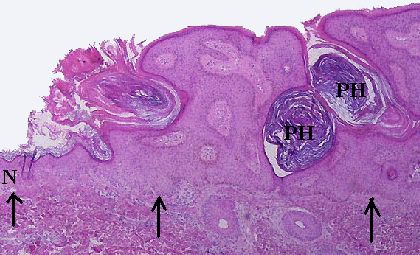
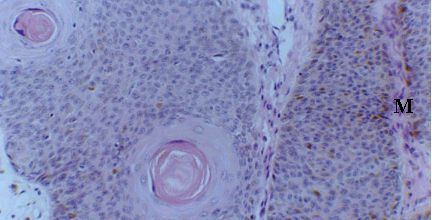
A seborrheic keratosis with an exophytic appearance.
The base of the lesion is
level (arrowed) with the normal epidermis (N) on the
left. Two pseudohorn cysts
(PH) are seen here which are formed from infoldings of
the epidermis. |
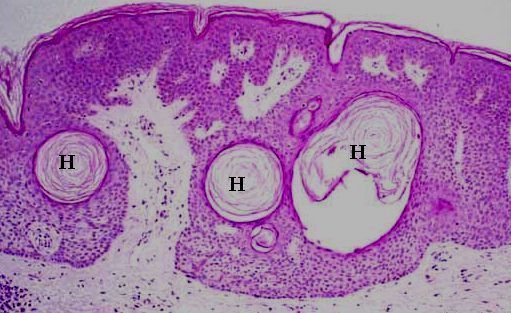
Seborrheic keratosis with horn cysts. |
Horn cysts and pigmentation in the basaloid cells of
seborrheic keratosis. |
Common viva questions:
-
What is the significant of actinic (solar) keratosis? (malignant transformation
to squamous cell carcinoma)
-
How can actinic keratosis be treated? (excision without clear margin if
localized, cryotherapy with liquid nitrogen or topical 5-FU)
-
Shown clinical pictures of basal cell carcinoma, squamous cell carcinoma,
actinic keratosis and seborrheic keratosis and discuss the significant
of each condition and treatment.
|