Ocular trauma is a common casualty referral. They can result from fight,
fall, foreign body at work or road traffic accident. It is important for
the referring doctor to differentiate blunt ocular trauma from perforating
ocular injuries. The latter may leave the eye with an open wound which
can lead rapidly to sight-threatening infection if not referred early.
Ocular trauma often has medicolegal implication, it is important for
the attending physician to keep a good record including the presenting
visual acuity.
Open
eye trauma

Penetrating eye injury requires immediate referral because
of the risk of devasting ocular infection.
Presentation:
-
Most commonly seen in children at play with sharp object
-
Shattered windscreen in road traffic accidents
-
High velocity missles at work place
Examination:
-
Visual acuity is reduced due to cornea distortion or blood
-
Most injuries involves the cornea or at the corneoscleral
junctions. Therefore displacement of the iris or pupil should alert the
possibility of open eye injury.
Management:
-
Refer the patient immediately to the eye casualty
|
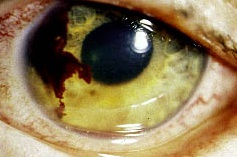
Figure 1.
This patient sustained a left peforating eye injury when
his friend threw him a sharp pencil at
school. The visual acuity was hand movement. Note the
displacement of the iris and pupil towards
8 O'clock where the perforation occurs at the corneoslceral
junction. He was admitted for wound
repair and was given antibiotic cover. The eventual visual
acuity
was 6/12 with glasses. |
|
Ocular
foreign body
Perforating eye injuries from foreign
body are uncommon. More commonly the foreign bodies are found in the subtarsal
area and cornea where there can be easily removed.
Presentation:
-
pain
-
red eye and
-
watery eye
Examination:
-
visual acuity is important, in the presence of severe pain
and blepharospasm visual acuity is checked after instillation of topical
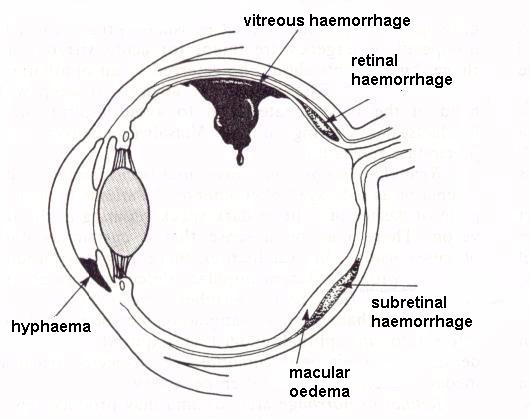
anesthesia. Intraocular foreign body can cause drop in visual acuity through
cataract or vitreous haemorrhage
-
note any distortion of the pupil or iris which may be caused
by a perforating injury
-
eversion of the upper lid is essential as foreign body may
be lodged in the subtarsal area causing corneal abrasion
Management:
-
subtarsal or corneal foreign bodies can easily be removed
with a cotton bud following instillation of topical anesthesia.
-
refer patient within 24 hours if the corneal foreign body
cannot be easily or completely removed.
-
any patient with suspected intraocular foreign body should
be referred immediately. History suggestive of intraocular foreign body
include the use of hand-hammer on metal or accidnts with industrial power
tool
 |
Figure 1.
Metal corneal foreign body. This can be easily removed
with a cotton bud after
application of topical anesthesia. |
 |
Figure 2
A painful eye caused by a subtarsal foreign body. Eversion
of the upper lid reveals the
foreign body which may otherwise be missed. |
 |
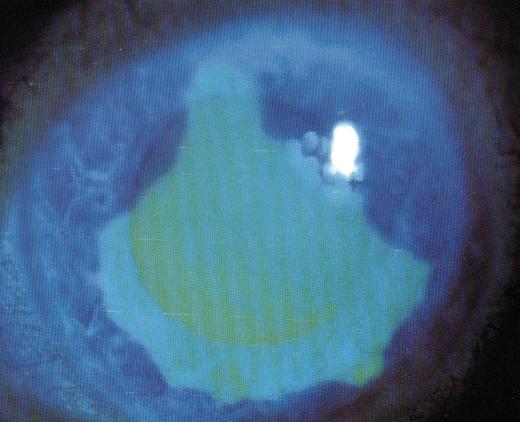
Figure 3
This welder sustained a penetrating injury at work. The
picture shows a piece
of iron foreign body embedded in the vitreous. This was
removed within 24
hours by the vitreoretinal surgeon. Intraocular iron
is toxic to the eye tissue
and should be removed. |
Return to the top
|
|