Retinoblastoma is the most common primary ocular tumour in
childhood. It is also a favourite topic of the examiners as they can test
the candidates' knowledge of genetics.
If you were given a gross pathology of the eye, comment on the following:
-
the size of the tumour
-
the location of the tumour (endophytic or exophytic; single
or multiple; any vitreal seedings)
-
any spread outside the globe (especially of the optic nerve.
In optic nerve involvement, there may be abnormal optic nerve enlargement
or tumour surrounding the nerve. Extraocular spread is of great prognostic
value.)

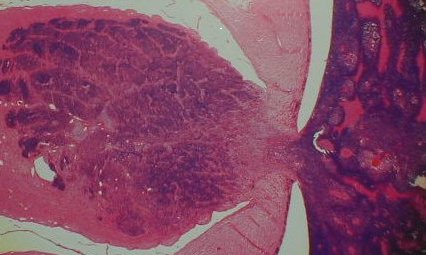
An endophytic retinoblastoma. The tumour grows
into the vitreal cavity. (In exophytic type, the
tumour grows into the subretinal space). |

Optic nerve (O) invaded by retinoblastoma (R). |
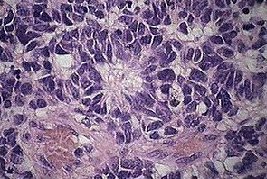
Under the microscope, retinoblastoma contains deep blue cells
with little cytoplasm. As the tumour cells usually outgrow their blood
supplies, necrosis and haemorrhage are common within the tumour.
In the slide, you will be expected to comment on:
-
differentiation of the tumour (although this is of little prognostic value)
-
any presence of tumour in the optic nerve.
|
 |
Flexner Wintersteiner rosettes:
clusters of cuboidal or short columnar cells arranged around a central
lumen. The nuclei are
displaced away from lumen. |
|
 |
Homer Wright rosettes: radial
arrangements of cells around a central tangle of fibrils. (pseudorosette). |
|
 |
Fleurette (arrowed): photoreceptor differentiation. |
|
 |
Optic nerve (left) infiltrated
by retinoblastoma (right). Note the presence of retinoblastoma (dark blue)
in the optic nerve substance. |
The following features are commonly seen in all retinoblastomas:
-
necrosis with islands of retinoblastoma
-
staining of the blood vessels ( from the release of the DNA
from necrotic retinoblastoma)
-
calcification
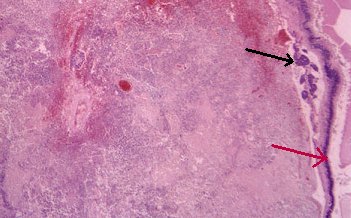 . . |
Necrosis and haemorrhage within the retinoblastoma. Residual
retinoblastoma (black arrow) appears as dark blue lesion next to the retina
(red arrow) |
 |
Retinal vessels surrounded by retinoblastoma. The vessel
walls are stained blue. The pink areas are the results of tumour necrosis. |
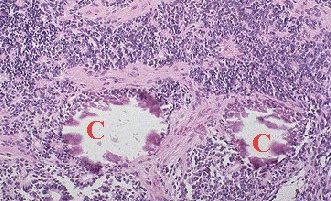 |
Retinoblastoma with areas of necrosis (the pink areas)
and two areas of calcification (C). |
Common viva questions:
-
What is the genetic of retinoblastoma?
-
What is the risk of retinoblastoma in a second child if the
first child has:
a. unilateral retinoblastoma;
b. bilateral retinoblastoma
and there is no family history of retinoblastoma?
-
What are the prognostic factors in retinoblastoma? Is Reese-Ellsworth's
classification useful for survival? (Extraocular spread is the main
factor that determine the prognosis. Survival rate is also affected by
the development of second tumour especially osteogenic sarcoma. Reese-Ellsworth's
classification is useful in predicting the tumour response to external
beam radiation but does not predict the survival rate.)
|